For an appointment about pain, symptoms, risks, and treatment contact us or to learn more about your world renown surgeons at Seattle Neuroscience Institute visit our home page.
Seattle Neuroscience Institute
Trigeminal Neuralgia Treatment
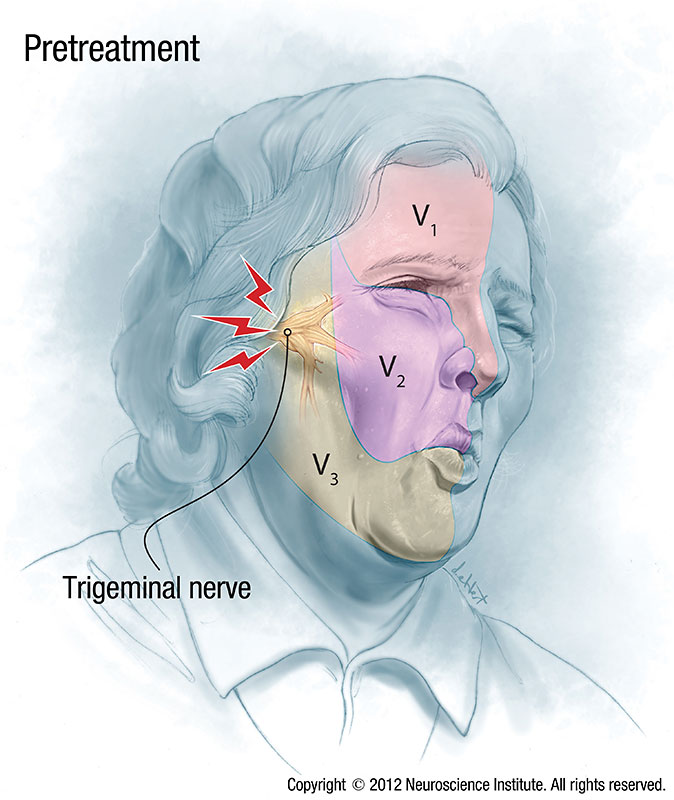
Trigeminal neuralgia, also called tic doloureux, is a condition characterized by episodes of intense facial pain that lasts from a few seconds to several minutes. Clusters of attacks can last for several hours. The pain occurs in areas of the face where the trigeminal nerve supplies normal sensation: cheek, nose, jaw, teeth, gums and lips, and the eye and forehead. This condition causes sudden, sharp and very severe pain, usually only on one side of the face. The pain is described by patients as feeling like stabbing, electric shocks, burning, crushing, exploding or shooting pain. People with this condition may initially experience short, mild attacks, but trigeminal neuralgia can progress, causing longer, more frequent bouts of pain. When severe repeated attacks of pain occur, those affected often have to stop what they are doing, sit down and usually cannot talk to others until the symptoms stop. If left untreated, the condition tends to worsen over time and require increasing doses of medications, although some patients can undergo spontaneous remission of symptoms over time. Trigeminal neuralgia affects women more often than men, and is more likely to occur in people over age 50.
Classic trigeminal neuralgia, or type 1 trigeminal neuralgia, has a number of clinical features. These include repeated sudden severe episodic pain attacks, which are in the distribution of the trigeminal nerve, restricted to one side of the face. These episodes usually have a trigger zone, or something which provokes the attack such as face washing, chewing, brushing teeth, a cold wind on the face, shaving, or eating. However, in many patients, the pain is generated spontaneously without any apparent stimulation. Most patients at the onset of symptoms, are pain free between the sudden attacks, and do not have permanent numbness in the face. Classic trigeminal neuralgia also is initially relieved either partially or completely, by certain anticonvulsant medications. These medications include phenytoin, carbamazepine, oxcarbazepine, gabapentin, and others. As the condition gets worse, patients can get a component of constant pain that persists in between the severe episodic pain attacks. If this constant aching or burning pain occurs as the most prominent feature patients are often given a diagnosis of atypical facial pain, or type 2 trigeminal neuralgia.
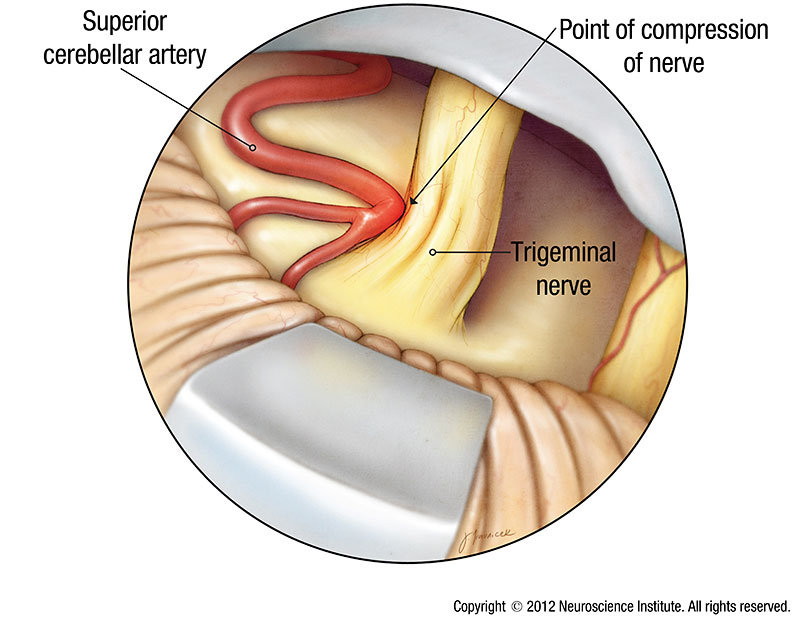
Trigeminal neuralgia causes include blood vessels pressing on the trigeminal nerve, which is the most common cause of trigeminal neuralgia, however in some cases the cause is unknown. The most common blood vessel to cause compression of the trigeminal nerve and trigeminal neuralgia is the superior cerebellar artery or a branch of this artery. On occasion one or more large veins can irritate or compress the nerve and cause the condition. These vessels can compress or irritate the nerve due to their pulsations or pressure changes between where the nerve exits the brainstem and where in enters the base of the skull. In rare instances tumors along the pathway of the trigeminal nerve at this or other locations may be responsible for trigeminal neuralgia. In some cases trigeminal neuralgia can be associated with multiple sclerosis.
Because the condition may be confused with other craniofacial pain syndromes, it is important that patients seek the opinion of a trigeminal neuralgia specialist to help make the diagnosis. Trigeminal neuralgia specialists are usually neurologists or neurosurgeons, otolarygologists or craniofacial pain specialists. Other conditions may mimic trigeminal neuralgia including temporomandibular joint pain or jaw pain, sinus infections or other sinus conditions, dental conditions including cavities, infections needing root canals, hypersensitive teeth, and other dental pathology. Occasionally patients have undergone root canals, tooth extractions, or other dental procedures in attempts to treat trigeminal neuralgia symptoms, which in retrospect had arisen from the trigeminal nerve itself.
In addition to the clinical symptom description, imaging studies are also utilized, most commonly high resolution MRI of the brain with and without intravenous contrast, and occasionally head CT. Even though a vascular compression is the most common cause, it is important to rule out tumor, multiple sclerosis, skull base lesions, infections, sinus pathology, temporomandibular joint, and jaw pathology. The finding of vascular compression of the trigeminal nerve on MRI is not 100% reliable in determining of the cause of symptoms for several reasons. The current MRI scans in use are not of sufficient resolution to determine if the nerve is compressed or just lying next to a blood vessel. It also may be difficult to determine if an adjacent blood vessel to the trigeminal nerve is an artery or a vein, and whether or not it is causing irritation and hyperexcitability of the nerve, which is usually the cause of the symptoms.
Trigeminal neuralgia treatment options include medical management using carbamazepine, oxcarbazepine, gabapentin, phenytoin, lioresal and others. If patients experience incomplete relief of symptoms, side effects, or toxicity from medications, then other treatments including trigeminal neuralgia surgery, or radiosurgery for trigeminal neuralgia can be effective. Trigeminal neuralgia surgery most commonly involves microvascular decompression of the trigeminal nerve which is an operative procedure to protect the nerve from irritation by a surrounding blood vessel. Other trigeminal surgery options involve neurolysis, which is partial damage to the nerve by injection of alcohol, balloon compression, or heating/burning with radiofrequency by passing a probe through the cheek into the trigeminal nerve.
Symptoms
- Intermittent severe episodic pain on one side of the face or teeth
- Symptoms may involve the eye, mid face or the lower face, or all regions at once
- Usually there are pain free intervals in between the attacks of severe pain
- Sometimes the symptoms are triggered by chewing or touching the face or even wind on the face
- There is usually normal sensation on the face
Causes
Trigeminal neuralgia in some cases doesn’t have a specific cause. The most common known causes are conditions that can irritate the trigeminal nerve
- A blood vessel pressing on the trigeminal nerve is the most common cause
- Tumor (rare)
- Multiple sclerosis
- Unknown
Risk Factors
Trigeminal is more common in middle-aged and elderly women. The mean age of onset is approximately 40 years old.
Diagnosis
Your doctor will ask about your symptoms and medical history. A physical exam will be done. Tests may include:
- An MRI of the brain
- Evaluations of the teeth or temporo-mandibular joint
Prevention
There are no current guidelines to prevent trigeminal neuralgia.
Treatment
Because of the variety of treatment options available, doctors usually can effectively manage trigeminal neuralgia with medications, injections or surgery. Treatment usually starts with medication. However, over time, some patients eventually stop responding to medications, or may experience unpleasant side effects. For those people, injections or surgery provide other treatment options. Other treatment options for trigeminal neuralgia include alcohol injection, glycerol injection, balloon compression of the trigeminal nerve, radiofrequency thermal rhizotomy, and surgical rhizotomy, which means partially damaging the nerve.
Medication
Medications are used to lessen or block the pain signals sent to your brain, and are the most common initial treatment for trigeminal neuralgia. Some medications include anticonvulsants or antispasmodic agents.
Microvascular Decompression Surgery
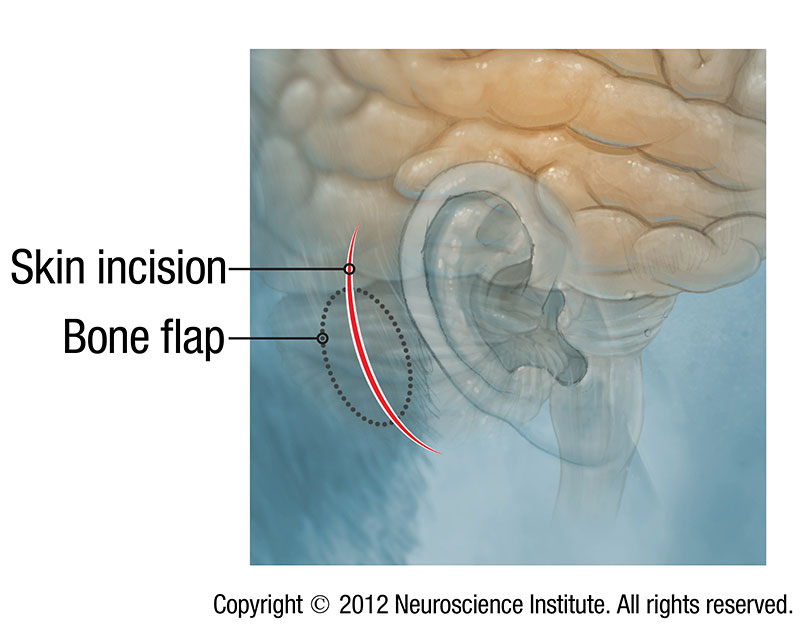
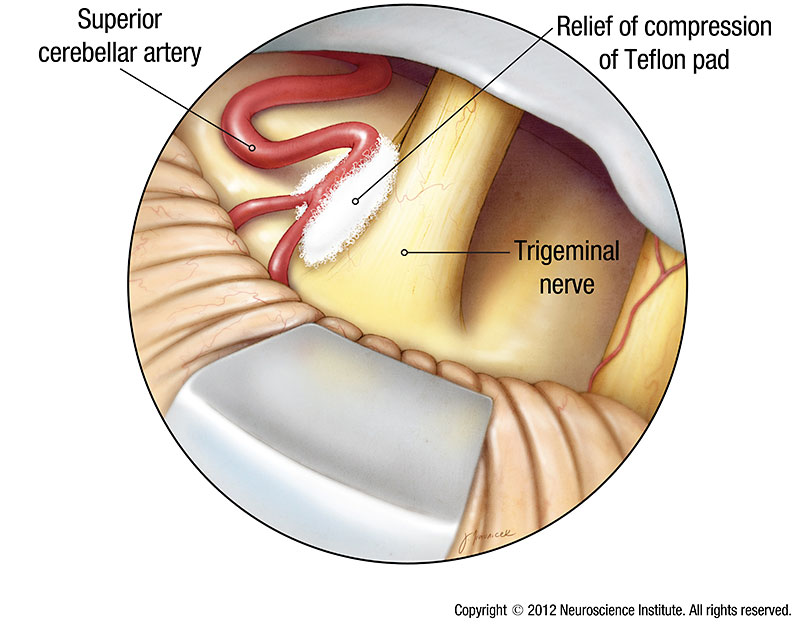
Microvascular decompression is a delicate procedure that is performed through a small opening behind the ear. The goal of this procedure is to prevent a blood vessel from compressing the trigeminal nerve. The surgery is performed under general anesthesia.
Through this small opening, the neurosurgeon uses a powerful microscope to view the trigeminal nerve. From here, the surgeon meticulously separates the nerve from the artery that is pressing against it. To relieve the pressure, the surgeon inserts a Teflon® pad between the artery and the nerve, keeping the artery from touching the trigeminal nerve.
To make sure that other nerves are not damaged by the surgery, the surgeon carefully monitors nerve function of the facial and acoustic (hearing) nerves. This is done by gently inserting tiny electrodes (metal wires that conduct mild electrical signals) into the muscles around the eye and mouth.
After the Procedure
Following the decompression procedure, the neurosurgeon closes the bony opening behind the ear, and you will be awakened and allowed to recover from anesthesia. Once this pressure has been relieved, patients often report immediate and complete relief from the pain. Most people stay in the hospital for observation for 2 days after surgery. Pain relief is usually immediate and medications are gradually discontinued over a two- week period following surgery.
Durability
The microvascular decompression procedure in patients with classic or type 1 trigeminal neuralgia has been shown to be the most durable treatment over long term follow up in studies that have followed patients for over 20 years.
Long term durability of microvascular decompression for trigeminal neuralgia
Radiosurgery
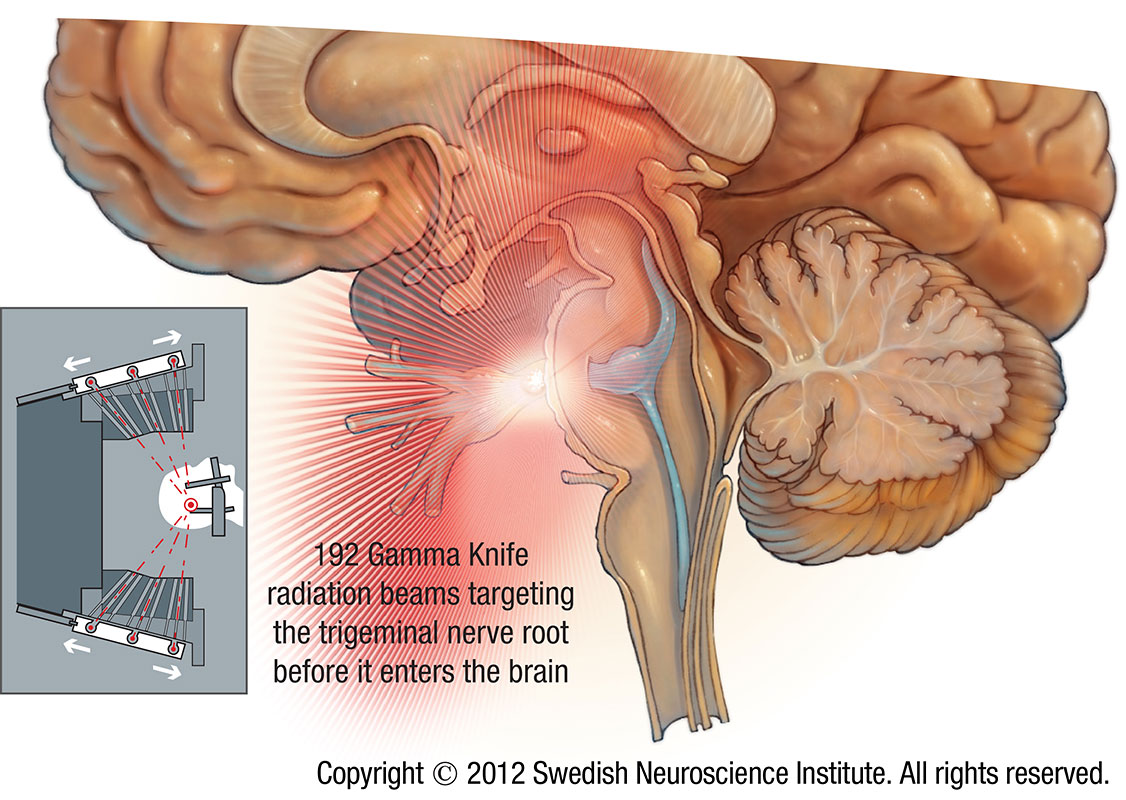
Another treatment option for trigeminal neuralgia is radiosurgery. Gamma Knife radiosurgery involves delivering a focused, high dose of radiation to the root of the trigeminal nerve. This treatment uses radiation to damage the trigeminal nerve and reduce or eliminate pain. Relief occurs gradually and can take several weeks to begin.
There are certain reasons why Gamma Knife may be a good treatment option to consider.
- There are medications that are used to control trigeminal neuralgia. Each of the drugs, however, has side effects that may be difficult to live with. If you experience side effects to medications or have used these medications and can no longer cope with the side effects, Gamma Knife may be an alternative treatment.
- Gamma Knife radiosurgery allows the patient to avoid general anesthesia, an incision in the scalp, and the risk of infection or other surgical complications. Radiosurgery also eliminates the need to shave the head in preparation for surgery, and recovery time is much shorter than the post-surgical hospital stay. Radiosurgery patients usually leave the Radiosurgery Center shortly after treatment and resume their normal daily activities.
- While some treatment options are safest for healthy, younger patients, Gamma Knife can be used to treat patients of any age, including the elderly, and to treat patients who may have other chronic medical conditions. Unlike surgery, there is no need to stop anti-coagulation (blood-thinning) medication prior to treatment.
The Gamma Knife procedure has several steps that occur on one day, including imaging, treatment planning and treatment. The treatment itself takes about one hour.
A unique treatment plan is created for each patient based on images that are taken just before treatment. The plan is used to program the Gamma Knife to send hundreds of beams of radiation from multiple angles and directions at the same time to the precise place where the trigeminal nerve exits the brain. This area is called the nerve root. It is the location of the cause of trigeminal neuralgia.
Alone each of those beams of radiation is not strong enough to damage normal brain through which it travels on its way to the target. Where the beams meet, however, the combined strength is enough to destroy the abnormal cells that case the pain of trigeminal neuralgia.
Once you have been diagnosed with trigeminal neuralgia, you and your doctor will discuss all of your treatment options. In planning your treatment, your doctor will consider your particular situation before making a recommendation.
Video
David Newell, M.D. talks about trigeminal neuralgia, who it affects, and how it’s treated.
Video demonstration of microvascular decompression of the right trigeminal nerve for trigeminal neuralgia. Surgery performed by David W Newell MD.
Warning: this video contains graphic depictions of neurosurgery.